Time for a bit of a personal COVID epistemic update. To reiterate: I’m no expert, and while there’s no shortage of those, plenty of folks keep asking what I think.
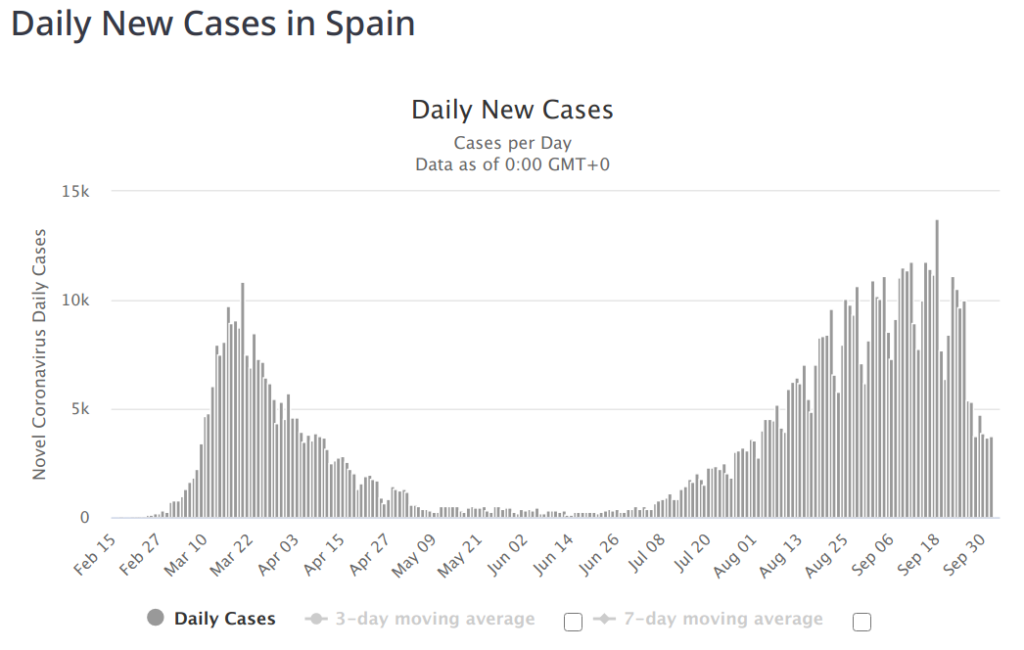
First, let me talk about the things it looks like I may have been wrong about. I’ve been pretty loudly claiming that the low-threshold herd immunity people are on to something. I think they still are, but I said early on that I’d seriously reevaluate their claims once we saw significant second-wave infections in places that were hard-hit initially. And now we have. First up was Spain:
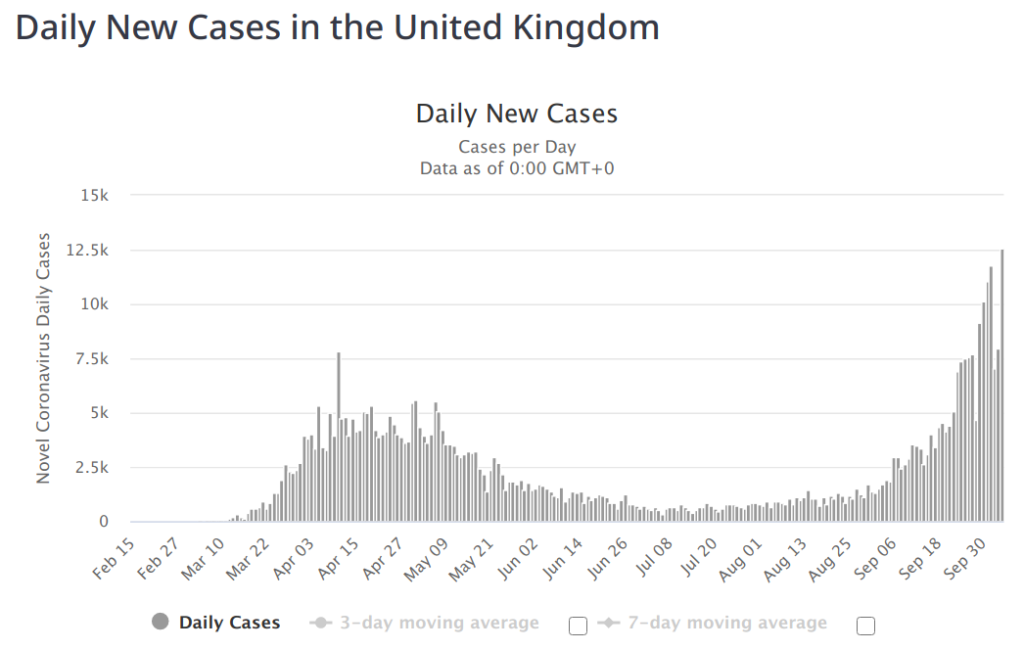
That alone is enough to make me question. But we’ve also got the UK:
My first thought is that it would be very interesting to break these things down by region. I spent awhile trying to do that for Spain, only realize the Spanish numbers are a giant mess, with a huge shift in record keeping between the two waves. My thought was that it’s possible that the hard-hit regions initially (Barcelona) shifted to a different region (Madrid) in the second wave. Maybe, but I don’t think it’s enough of an effect to matter. I couldn’t find much data to support the theory in Spain, and found nothing to support the theory at all in the UK.
So what about other places that were pretty hard hit, but don’t seem to have a second wave? There’s plenty of those, too:
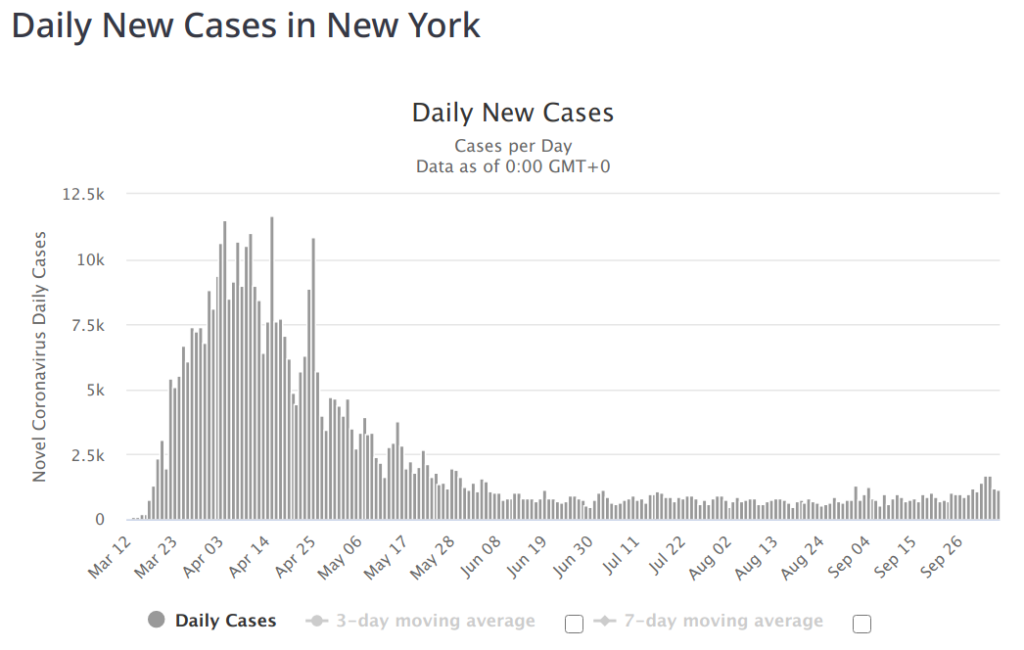
So, what’s different? My theory at this point is that the severe lockdown in Spain and the UK were effective at the beginning and halted the spread before we got to the herd immunity threshold. There’s some evidence to support this with seroprevalence studies. NYC saw seroprevalence as high as 22% in April, whereas Spain was more like 6% with similar numbers for the UK. Still hardly a smoking gun — we know these seroprevalence numbers aren’t very good. It matters a lot when you look as antibody numbers drop pretty quickly, especially after a mild infection. But, assuming (and it’s a questionable assumption) that the numbers are equally crap across countries, the higher numbers in NYC may well be significant.
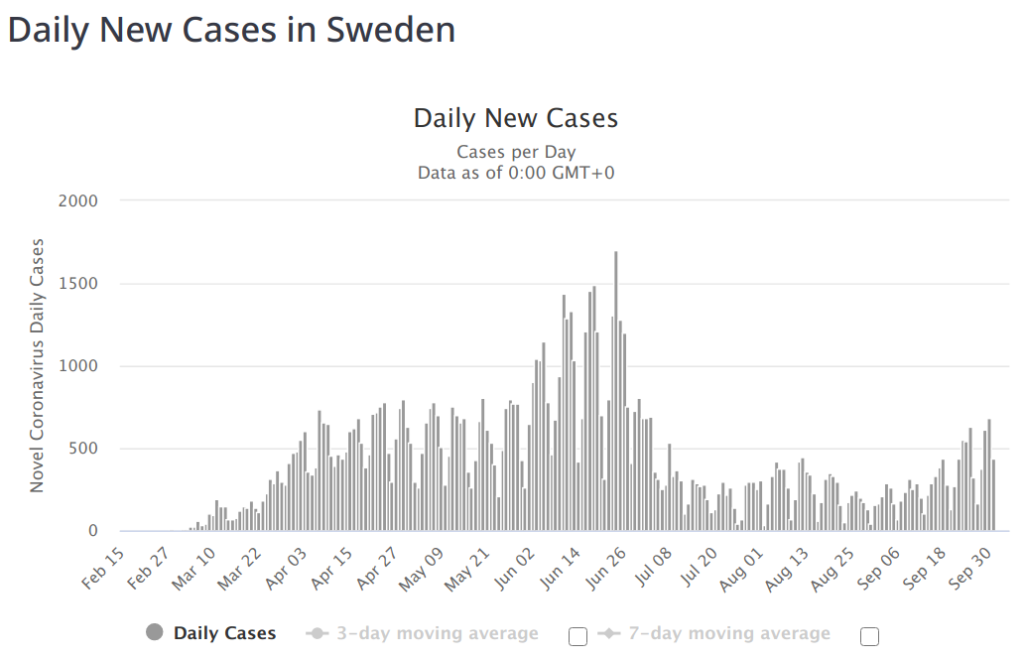
So, does this mean that “pursuing herd immunity” is a good strategy? Probably not, though I don’t think any country actually did that. Still, you can pick countries that did near-nothing and you see a curve that’s pretty familiar looking:
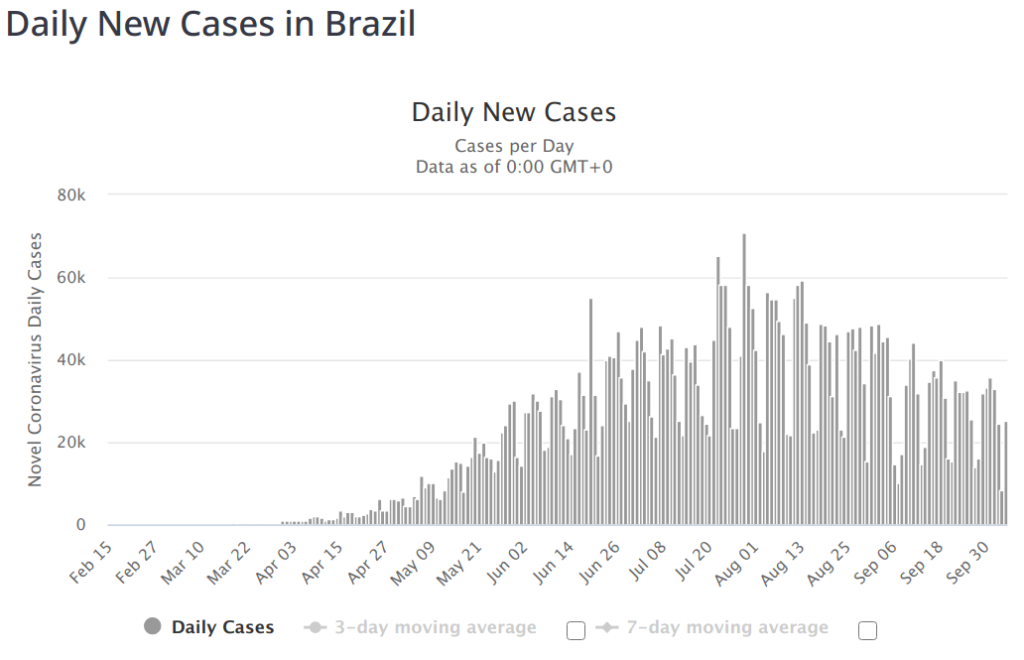
I think (though I don’t have much data to support this), that a Brazil-shaped curve is probably far better than a Spain-shaped curve. I think you can get a Brazil shaped curve with a much lower peak by enacting sensible measures that are far short of a lockdown. You know where this is going:
I think it’s starting to be pretty clear that in the long term, the total lockdown strategies should be judged a failure. They absolutely slowed the spread while countries were locked down, but I don’t see a significant benefit when you consider the post-lockdown bounce. And you must consider the post-lockdown bounce.
Why lockdown? The lockdowns were initiated with the idea that they’d keep healthcare systems from being saturated. They would “flatten the curve” — instead of overwhelming healthcare systems with uncontrollable, exponential growth, we could spread the inevitable infections out a bit so the healthcare system could manage it. In retrospect, however, I think it’s pretty clear that lockdowns weren’t actually necessarily to accomplish that goal. It became pretty clear early on that we’d accomplished that goal in the civilized west, but then, inexplicably the call shifted to, “crush the curve!”
The shifting goalposts lost me. It’s certainly possible to lockdown your way out of Coronavirus. It’s been successful in China and New Zealand so far, and it might even work in Australia. (If anyone wants to bet, my money is against it working in Australia long term, though they’ve done an amazing job so far.) But what about the U.S. or Europe? By the time we even considered it, it was too late.
The next-best argument for the lockdown is that we could use the time to stop the spread, set up test/trace/isolate, make lots of PPE, better align hospitals, etc. We certainly did none of this in the U.S. Germany implemented a super impressive sounding test and trace program…. how are they doing?
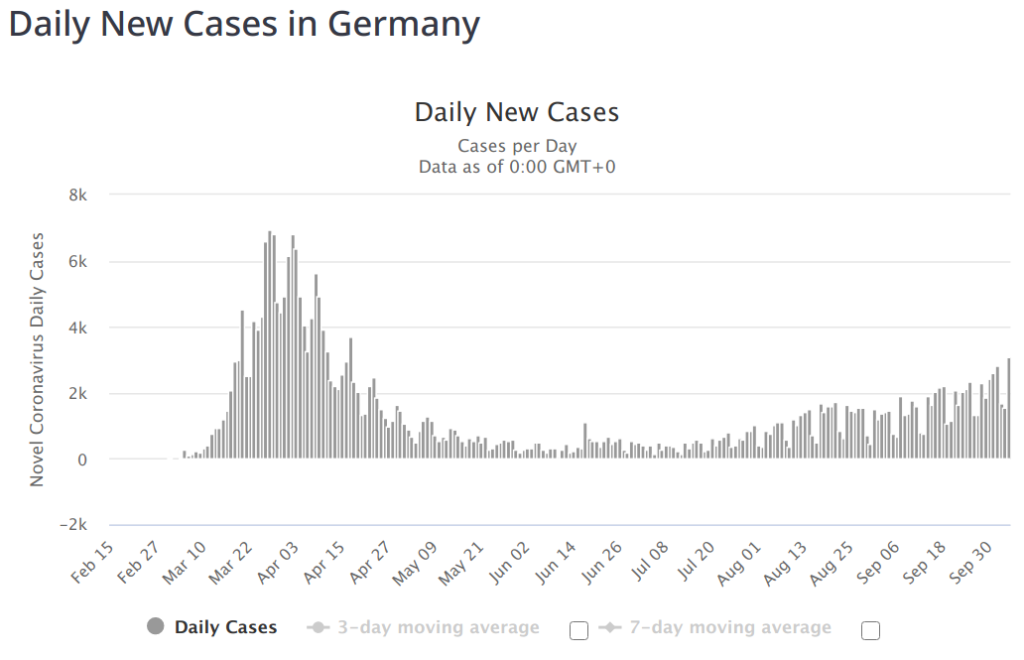
Yeah. That’s not looking like super-impressive results to me, but I think it’s too early to judge.
What else have I been wrong about? I predicted the whole country would look a lot like New York by October. I meant by the end of October, so technically, I guess I’ve got 30 days, but it’s not looking good.
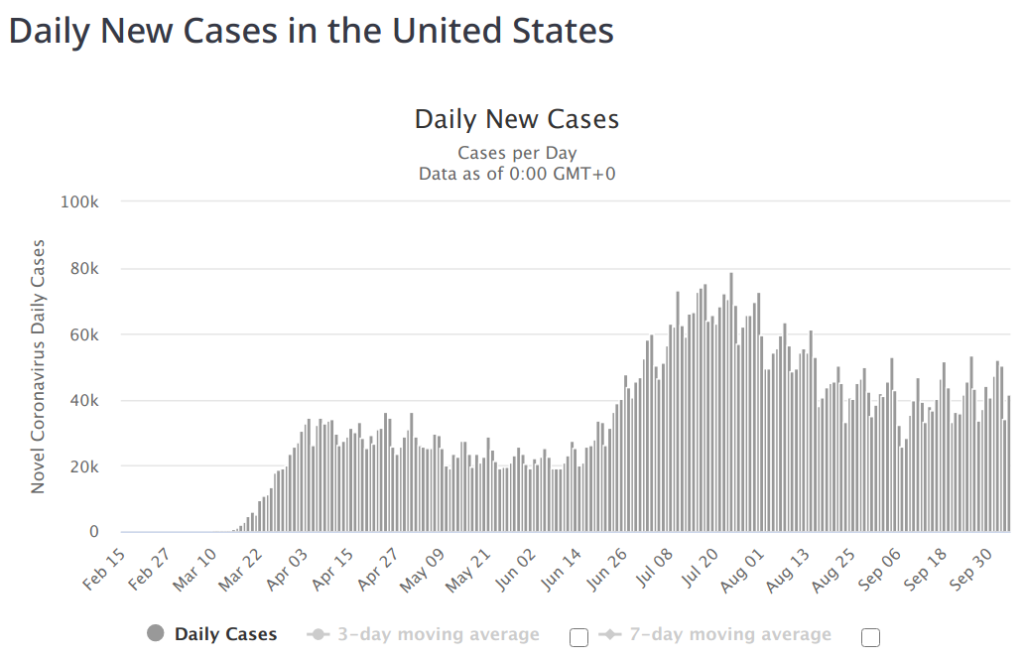
We know this graph is distorted. The April peaks should probably be closer to the 100k line if we had the testing then we’ve got now. But who cares–we haven’t see a huge testing ramp-up in the month of September when I’d have expected to start seeing a fall-off. The worst-hit states are showing improvement: California, Texas, Florida. But what about places like Illinois? Or Colorado? This is a huge country, and we spent a long time locked down. I think it’s going to take another couple months.
So what should we be doing? We should be investing heavily in rapid tests. Cheap, not-very-accurate rapid tests. Such tests have low false-negative rate, but a higher false-positive rate. But most importantly, they very rarely report negative when someone is highly contagious. Who cares how good PCR tests are if they’re expensive, hard to get, inexplicably involve shoving an unobtanium swab into your brain, and are so sensitive they can detect the virus long after you’re contagious? Imagine how much better the world would be if your fellow coworkers or students or friends could all take a daily test. It doesn’t have to be perfect, but if the White House were doing it regularly (and, you know, acting on the results), we wouldn’t be looking at the disaster they’ve got right now.
What about a vaccine? I’m amused that everyone who thinks this virus is a deadly, terrifying scourge also believes that we should NOT rush a vaccine. Really? I think the worse this thing is, the more we should discount the risks of a bad vaccine in favor of the potential benefits. I’m not entirely sure where the right balance is, but the dissonance is deafening. Also, we’ve got thousands of young people who have volunteered for human challenge trials, but a world that’s too queasy to take them up on it. Why? The modern world has never seen anything like this, and I think it’s silly to be so sure that standard vaccine trials are necessarily the right answer here.
Okay, but what about individual decisions? I think, at this point and for the near future, theaters, cinema and live music are dead and should stay dead. I think any gathering of more than a dozen people indoors is unnecessary and shouldn’t happen. I think at-risk folks should avoid everything. But what about us younger folk?
It depends. An 18-year-old living at home with a 65-year-old has, I think, a duty to not expose themselves to anything that the 65-year-old shouldn’t be exposed to. But what about people like me? I live with an old woman, it’s true, but she’s not yet in the at-risk category. Sure, it’s possible either of us could have long-term health consequences from a run-in with COVID. But those risks are quite rare, and we ride motorcycles, which is far more likely to have long-term health consequences.
Personally, I’m mostly going about my life as normal, but my life isn’t that normal. I’ll forgo my annual trip to the movie theater, but I really miss live music. I’m going to restaurants less frequently, but a lot of that is just because going to restaurants sucks right now. I see small groups of friends now and again, and that’s all I really want, anyway.
But I’m also not visiting my mother, and this is rough for her. She’s lonely and hasn’t socialized in forever, and unlike me, she likes people. But she’s old, moth-eaten, and high-risk. I’m just not going to be the one that kills her (unless she asks me to). I’m considering a 2-week self-quarantine and then hopping in my plane to fetch her for a visit…
I’m convinced of a couple of things: At least for the U.S., it’s going to get better from here, not worse. Also, we’re all getting it eventually.
{kind=link}
{kind=link}
Leave a Reply